Ischaemic Strokes of Different Etiologies
Stroke due to large artery atherosclerosis
A number of arteries that originate from the aorta supply our cerebral cortex. For example, the anterior circulation originates from the common carotid artery, which subsequently branches into the internal carotid artery and external carotid artery. Whilst the external carotid artery supplies the structures outside the cranium, the internal carotid artery subsequently forms the middle cerebral artery and anterior cerebral artery and provides blood supply to the frontal lobe, parietal lobe and part of the temporal lobe. In contrast, the posterior circulation originates from the vertebral arteries which subsequently form the basilar artery and posterior cerebral artery. A number of arteries branch out from the basilar artery such as the posterior inferior cerebellar artery, anterior inferior cerebellar artery and superior cerebellar artery and these supply the brainstem, cerebellum, occipital lobe as well as the inferior surface of the temporal lobe.
Occlusion of these large arteries may be due to atherosclerotic changes. This may be either due to plaque formation, with subsequent plaque rupture and formation of a thrombus directly occluding the artery. Or, the thrombus may dislodge and travel distally, occluding another artery (a phenomenon called artery-to-artery emboli).
Large artery atherosclerosis may also be subdivided into extra-cranial atherosclerosis or intra-cranial atherosclerosis. Extra-cranial atherosclerosis is where there are atherosclerotic changes involving the common carotid arteries, carotid bifurcation (also known as the carotid bulb), extra-cranial portion of the internal carotid artery, as well as the extra-cranial portion of the vertebral arteries. In contrast, intra-cranial atherosclerosis will involve arteries such as the anterior cerebral artery, middle cerebral artery, intracranial portion of the vertebral artery, basilar artery, posterior and anterior inferior cerebellar artery, superior cerebellar artery and posterior cerebral artery. It is useful to know that whilst extra-cranial atherosclerosis is much more common amongst Caucasians, atherosclerosis of the intra-cranial atherosclerosis is much more prevalent amongst Asians.
In addition to long tract signs (e.g. pyramidal distribution of weakness, sensory disturbances etc.), patients with stroke due to large-artery atherosclerosis usually also present with cortical signs (e.g. expressive and / or receptive dysphasia, sensory and / or visual inattention, visual field disturbances) or cerebellar dysfunction. The lesion on cranial imaging is usually >1.5cm and there is evidence of significant intra or extra-cranial atherosclerosis on vascular imaging (carotid or trans-cranial Doppler ultrasonography, CT or MR angiogram or digital subtraction angiography).
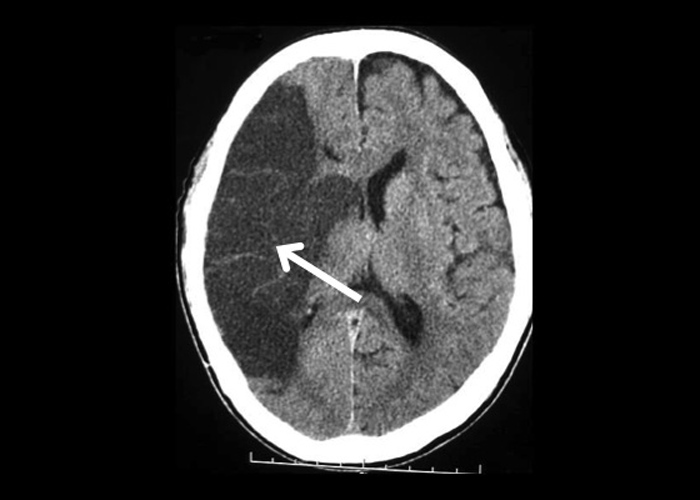
The neuroradiographs shown in this section are all from patients with ischaemic stroke due to large artery atherosclerosis. The first CT (Figure 1) is from a patient with underlying bilateral severe internal carotid artery atherosclerosis presenting with a bilateral watershed infarct after an episode of severe hypotension. The second CT (Figure 2) is from a patient with severe left internal carotid artery infarction and ischaemic changes could be seen could be seen in the territories supplied by the left anterior and middle cerebral arteries. The third CT (Figure 3) is from a right-handed patient with a past history of right middle cerebral artery infarction presenting at that time with sudden onset of left sided weakness as well as sensory inattention. In this particular patient, although carotid duplex ultrasound did not reveal evidence of extracranial atherosclerosis, a trans-cranial duplex ultrasound and subsequently magnetic resonance angiography of the circle of Willis (time of flight technique) confirmed that the patient had significant intra-cranial atherosclerosis involving the right middle cerebral artery. The last CT (Figure 4) is from a patient with a left posterior cerebral artery infarct. This patient presented with an acute onset of right homonymous hemianopia and subsequent CT angiography confirmed a severe stenosis of the left posterior cerebral artery.