

Ischaemic Changes of Different Anatomical Regions or Vascular Territories
Infarction involving the subcortical territory: Brainstem infarct
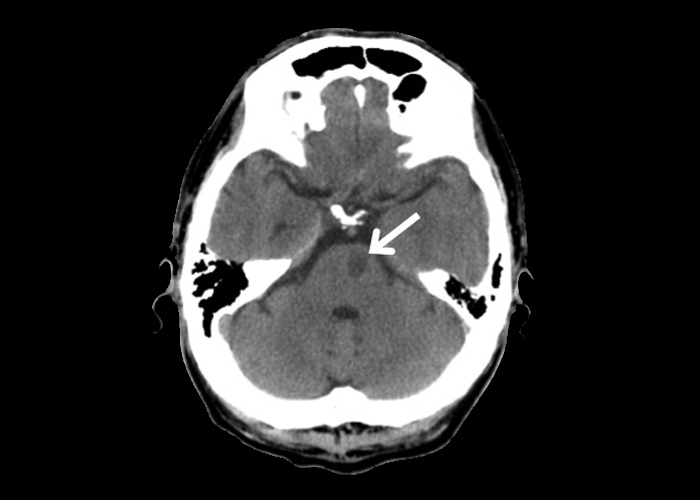
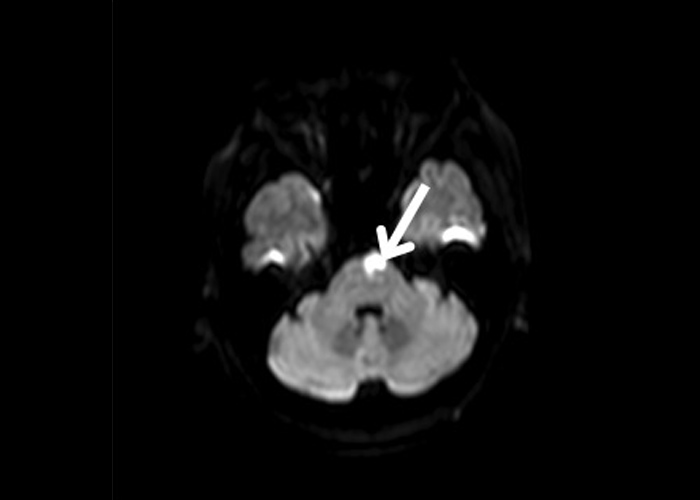
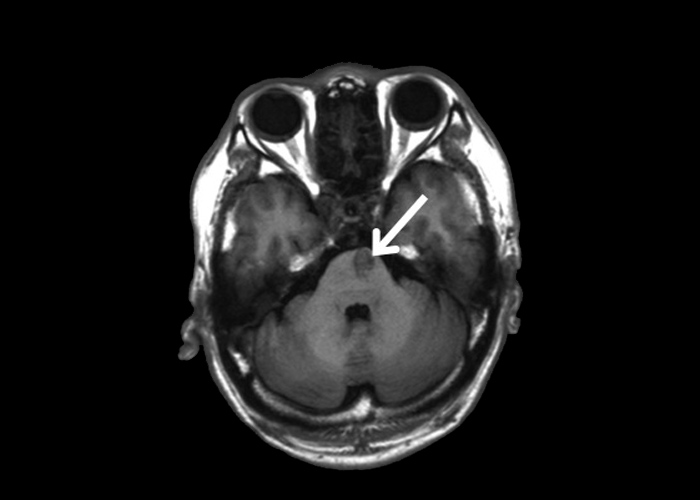
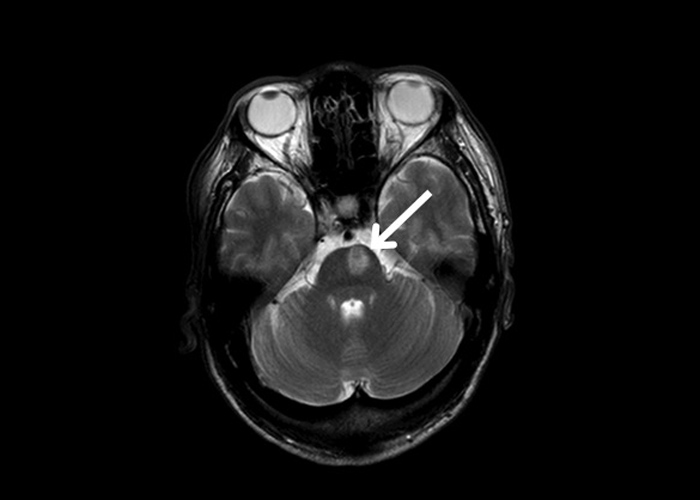
This patient presented with an acute onset of right-sided hemiparesis. A CT brain subsequently confirmed a left para-median pontine infarct ![]() (Figure 1). This was also demonstrated on cranial MRI, which showed an acute lesion with restricted diffusion on diffusion-weighted imaging (Figure 2). The lesion was hypointense on T1 (Figure 3) and hyperintense on T2 sequence (Figure 2) of MRI, all of which suggests an ischaemic event.
(Figure 1). This was also demonstrated on cranial MRI, which showed an acute lesion with restricted diffusion on diffusion-weighted imaging (Figure 2). The lesion was hypointense on T1 (Figure 3) and hyperintense on T2 sequence (Figure 2) of MRI, all of which suggests an ischaemic event.
The subsequent set of non-contrast CTs demonstrates a para-median pontine infarct, this time of the right side ![]() (Figure 5). As the lateral corticospinal tract originates from the motor cortex, travels along the corona radiata, posterior limb of the internal capsule, midbrain, and pons before decussating at the medulla; patients with a midbrain or pontine infarct may therefore present with a sudden onset of contralateral weakness. The presence or absence of cortical, brainstem and sensory signs are therefore important in locating the lesion in someone presenting with an acute hemiparesis.
(Figure 5). As the lateral corticospinal tract originates from the motor cortex, travels along the corona radiata, posterior limb of the internal capsule, midbrain, and pons before decussating at the medulla; patients with a midbrain or pontine infarct may therefore present with a sudden onset of contralateral weakness. The presence or absence of cortical, brainstem and sensory signs are therefore important in locating the lesion in someone presenting with an acute hemiparesis.

The final set of scans are from a patient who presented with an acute onset of vertigo, right sided weakness, sensory loss over the right face and over the left side of the body. There was in addition dysarthria, dysphagia, a right Horner’s syndrome as well as right-sided ataxia. The clinical presentation suggests an acute right lateral medullary syndrome and is confirmed by a cranial MRI demonstrating an ischaemic lesion at the right lateral medullary region ![]() which is restricted in diffusion on diffusion-weighted imaging (Figure 6) and hyperintense in T2 (Figure 7).
which is restricted in diffusion on diffusion-weighted imaging (Figure 6) and hyperintense in T2 (Figure 7).







